June 29, 2026
Strategic Compliance Training for Employees GuideOur strategic guide helps Canadian businesses develop effective compliance training for employees. Scope, build, deliver, & measure impactful programs for 2026.
Read Full Post%20(1).webp)
Usman Malik
Chief Executive Officer
June 30, 2026

A clinic manager in Ontario gets the same questions every week. Can staff access records from home? Is the U.S. telehealth vendor acceptable? What happens if a physician downloads patient files to a laptop and that device disappears? None of those questions are abstract. They affect patient trust, operations, and legal exposure on the same day.
That's why healthcare IT compliance can't sit in a policy binder or live only with the IT team. In practice, it touches scheduling, clinical workflows, procurement, cloud architecture, cybersecurity, vendor management, and incident response. It also gets harder when a Canadian provider handles U.S. patient data, because the rules don't line up neatly.
A common scenario looks harmless at first. A Canadian clinic adds a U.S.-based specialist network, stores notes in a cloud platform, and gives administrators broader access than they need because it's faster during a busy week. Then a breach investigation starts. Leadership discovers the issue isn't only whether data was exposed. It's also whether access was properly limited, whether audit records exist, whether consent was valid, and which law applies to which patient record.
The scale of healthcare breaches shows why this matters. From 2009 to 2022, the United States reported 5,150 healthcare data breaches involving 500 or more records each, exposing over 382 million medical records in total, according to MedStack's review of healthcare compliance laws. Those figures are U.S.-specific, but they're a sharp warning for Canadian organisations handling cross-border patient data.
Most healthcare leaders aren't struggling because they don't care about compliance. They're struggling because compliance requirements collide with real operational pressure.
Practical rule: If a control only exists on paper and staff can bypass it in a normal workday, it won't protect you during an audit or after an incident.
What works is a defensible system. Access is role-based. Logs are preserved. Vendors are reviewed before procurement. Privacy and security teams work from the same playbook.
What doesn't work is treating healthcare IT compliance as an annual checklist. In healthcare, a small shortcut often becomes a large reporting problem later.
Leaders usually hear the acronyms first and the practical meaning second. That order should be reversed.
HIPAA applies in the United States and governs protected health information handled by covered entities and their business associates. PIPEDA is Canada's federal private-sector privacy law. PHIPA is Ontario's health privacy law and is often the most operationally important framework for Ontario providers because it focuses directly on personal health information.
This visual helps frame the split between federal and provincial obligations.
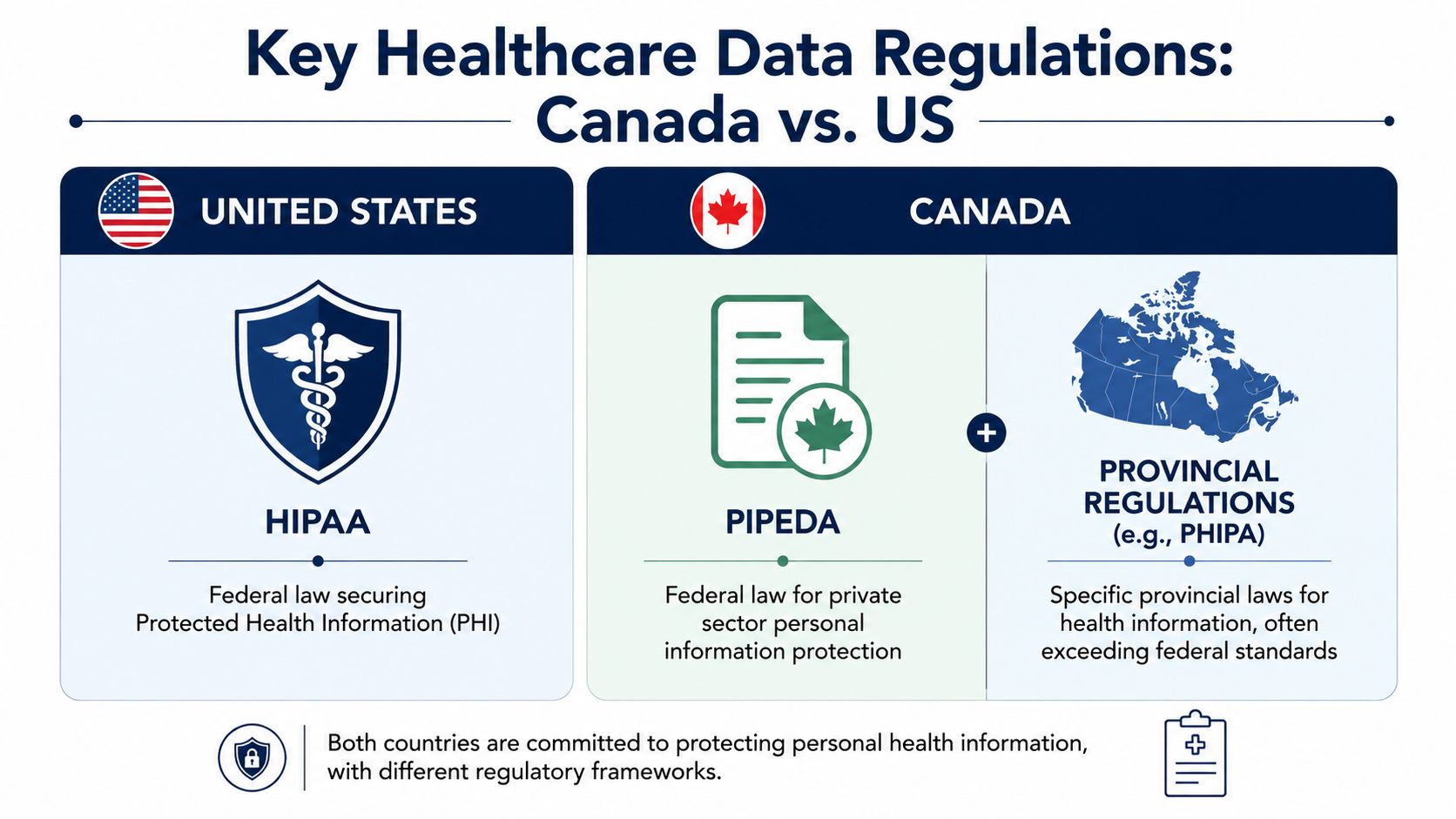
HIPAA is built around privacy, security, and breach obligations for the U.S. healthcare ecosystem. PIPEDA governs how private-sector organisations collect, use, and disclose personal information in Canada where applicable. PHIPA is narrower in one sense and stricter in another. It centres on health information custodians and the handling of personal health information in Ontario.
For technical teams, PHIPA matters because it speaks directly to controls. Ontario's PHIPA mandates strong technical safeguards including end-to-end encryption with AES-256 for data at rest and TLS 1.3+ for data in transit, role-based access control, and tamper-proof audit logging, with penalties for non-compliance reaching up to $500,000 for organisations, as outlined in this Digital Health Canada compliance guide.
When organisations use data for analytics, model training, or product improvement, teams also need to understand techniques such as anonymizing training data so secondary use decisions don't drift into privacy violations.
For a practical starting point on U.S. obligations, CloudOrbis has also published a HIPAA compliance checklist for Canadian organisations.
| Aspect | HIPAA (US) | PIPEDA (Canada - Federal) | PHIPA (Ontario) |
|---|---|---|---|
| Primary scope | Protected health information in the U.S. healthcare system | Personal information in private-sector commercial activity | Personal health information in Ontario healthcare settings |
| Typical covered parties | Covered entities and business associates | Private-sector organisations subject to federal privacy law | Health information custodians and related agents |
| Core focus | Privacy, security, permitted uses, breach obligations | Fair collection, use, disclosure, and accountability | Consent, custody, access, disclosure, and health-specific safeguards |
| Technical expectations | Administrative, physical, and technical safeguards | Appropriate safeguards based on sensitivity | Explicitly strong controls for encryption, RBAC, and audit logging |
| Consent model | More operational flexibility in healthcare use and disclosure | Consent-based privacy framework | Often more explicit and contextual for health information |
| Breach handling | U.S. healthcare-specific obligations apply | Canadian federal privacy obligations may apply depending on context | Ontario health privacy obligations apply in healthcare contexts |
The biggest mistake isn't misunderstanding definitions. It's assuming a U.S.-ready environment automatically satisfies Canadian requirements. It often doesn't. A system can be configured to meet HIPAA-style controls and still fail around consent, documentation, role design, or auditability under PHIPA.
Legal requirements become manageable when you translate them into safeguards. In day-to-day operations, healthcare IT compliance rests on administrative, physical, and technical controls. If one pillar is weak, the other two usually can't compensate for it.

Administrative safeguards are the decisions that shape everything else. They include risk assessments, access approval processes, workforce training, vendor reviews, policy management, and incident response planning.
These controls often fail unnoticed. A clinic may buy secure software and still fail because nobody documented who approves access, how often privileges are reviewed, or what happens when a staff member changes roles.
A useful administrative baseline includes:
Physical controls still matter even in cloud-heavy environments. Workstations in exam rooms, shared front-desk devices, open server closets, printed records, and unsecured laptops all create risk.
In healthcare settings, physical safeguards should be simple enough that staff will follow them under pressure.
Compliance breaks fastest at the point where a rushed employee can take a shortcut without anyone noticing.
Many organisations understandably prioritize this. In 2024, the number of individuals affected by large healthcare data breaches surged by 58%, highlighting the need for controls like MFA, RBAC, and automated encryption, according to HIPAA Journal's breach statistics analysis.
The most defensible technical stack usually includes MFA for clinicians and administrators, RBAC tied to job function, centralised logging, endpoint detection, encrypted backups, and secure remote access. Organisations building analytics or research workflows should also understand protected health information de-identification so they don't overexpose identifiable records unnecessarily.
Cloud architecture matters too. If your environment is fragmented across unmanaged SaaS tools, on-premise file shares, and personal devices, your controls won't behave consistently. Such conditions make a structured approach to cloud data protection in regulated environments operationally useful.
The most common bad assumption in this space is simple. If a Canadian provider is HIPAA compliant, that should cover U.S. patient data. It doesn't.
The gap usually appears around consent. HIPAA allows certain uses and disclosures within the U.S. healthcare framework that feel routine to American operators. Canadian health privacy law, particularly in Ontario, can require a more explicit and context-sensitive approach. That creates risk when the same workflow is applied to both populations.
A clinic might collect patient information for treatment, then later use portions of that data for internal quality review, referral coordination, analytics, or a new digital service. Under one framework, the workflow may appear acceptable. Under another, the organisation may need clearer consent language, narrower disclosure rules, or stronger documentation of purpose.
That's not a niche issue. Recent data shows that 73% of Canadian firms handling U.S. health data face compliance gaps due to conflicting patient consent rules, and 40% of Canadian healthcare IT breaches stem from these misaligned consent protocols rather than technical failures, according to SOC 2 Auditors' analysis of HIPAA in Canada.
The answer isn't choosing HIPAA or PHIPA. It's building workflows that recognise both.
For organisations that operate across provinces as well, local obligations can complicate things further. Even outside healthcare, sector-specific requirements show why regional compliance design matters. A useful example is this CloudOrbis article on IT compliance needs in Alberta private career colleges, which shows how organisations can't rely on one generic compliance template.
Most organisations already know they need better controls. The primary challenge is sequencing the work so it doesn't stall halfway through. Treat healthcare IT compliance as a managed programme, not an emergency project.
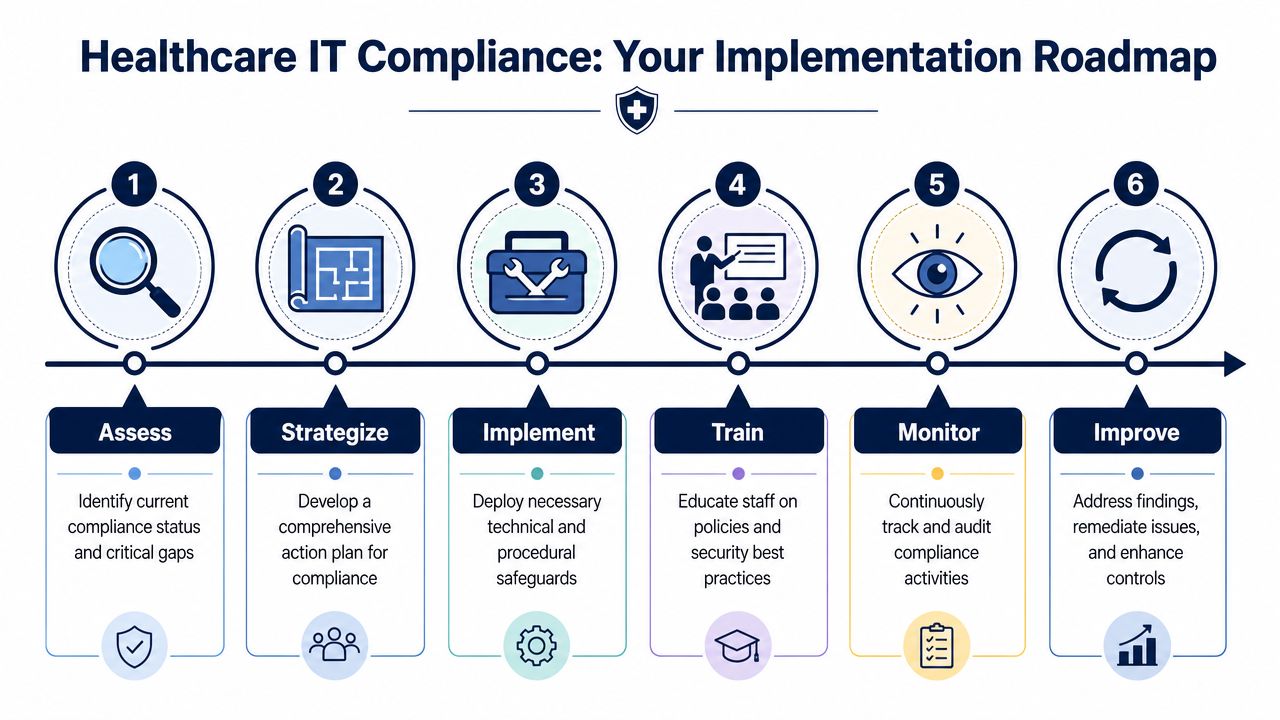
Assess your current state
Inventory systems, vendors, devices, data repositories, remote access paths, and user roles. Most compliance efforts fail early because nobody has a reliable map of where patient data lives.
Build a gap analysis
Compare current controls against your legal and operational obligations. Include policy gaps, logging gaps, weak vendor governance, and consent workflow issues.
Set governance before buying tools
Decide who approves access, who signs off on vendors, who owns incident response, and who maintains the evidence trail. Technology won't fix an ownership problem.
Field-tested advice: Start with identity, logging, and vendor review. Those three areas expose weaknesses quickly and give leadership a clearer remediation path.
Implement controls in the right order
Put MFA, encryption, RBAC, endpoint protection, backup controls, and secure remote access in place before you expand digital workflows. If you're relying on a service provider, make sure they can support healthcare-specific security and compliance operations. For example, CloudOrbis Inc. provides managed IT support, cybersecurity, compliance support, and strategic IT guidance for Canadian organisations that need help operationalising these controls.
Train the whole workforce
Training should reflect actual workflows. Reception staff, clinicians, finance staff, and administrators don't face the same risks. Tailor the training and document completion.
Monitor and improve continuously
Review access rights, investigate suspicious activity, test response plans, and update controls when your business changes. New clinics, new devices, and new vendors all alter your compliance posture.
A good roadmap is boring in the best way. It produces documented approvals, predictable access reviews, repeatable onboarding and offboarding, and logs that support investigations. It doesn't depend on one person remembering how things are supposed to work.
Audit readiness isn't built the month before an audit. It's built in the ordinary weeks when staff are provisioning accounts, renewing vendor contracts, responding to incidents, and updating policies.
The pattern behind many failed audits is familiar. Controls may exist, but evidence doesn't. Leadership believes access is restricted, but nobody can produce a documented approval trail. The organisation says vendors were assessed, but procurement files don't show it.
Benchmark data indicates that 78% of healthcare organisations that failed compliance audits in 2025 lacked documented access control policies or third-party risk evaluations, a foundational requirement under PHIPA and PIPEDA, according to Omega Systems' guide to IT compliance in healthcare.
That finding matches what shows up in practice. Common pitfalls include:
If your environment includes custom applications, patient portals, or internal automation, periodic code review matters too. A specialised AI code security audit can help identify security weaknesses in software logic and implementation before they become compliance issues.
Use internal reviews to test whether your stated controls can be proven. Ask simple questions. Who approved this access? Where is that record? Which vendor assessment supports this system? When was this policy last reviewed? The same discipline that strengthens privacy impact work also improves healthcare audits. This is why structured assessments such as a privacy impact assessment process in Alberta are useful models even beyond one province.
Auditors rarely discover brand-new problems. They usually uncover problems the organisation already suspected but never documented or resolved.
Most mid-sized healthcare organisations don't have the internal capacity to monitor every endpoint, review every security event, assess every vendor change, maintain audit evidence, and keep cross-border privacy obligations aligned. That's why compliance often slips between annual reviews.
A managed service model changes the operating rhythm. Instead of treating healthcare IT compliance as a periodic project, the organisation builds ongoing monitoring, maintenance, and remediation into normal operations. That matters because healthcare environments change constantly. Staff join and leave. New clinics open. Vendors add integrations. Remote access expands. Every change affects risk.

A useful managed IT relationship should cover more than ticket resolution.
The best arrangements also reduce friction between technical controls and clinical reality. MFA rollout, secure remote access, device encryption, and log retention all need to work in fast-moving healthcare environments. If they're designed without workflow awareness, staff will work around them.
For organisations weighing this model, this overview of managed IT services and security controls is a practical place to start.
Healthcare leaders don't need more acronyms. They need a compliance model that survives busy clinics, vendor changes, and cross-border data handling. That takes governance, technical discipline, and ongoing operational support.
If your organisation needs a clearer path through Canadian and U.S. healthcare compliance requirements, CloudOrbis Inc. can help you assess current risks, strengthen safeguards, and build a practical compliance operating model that fits the way your teams work.
June 29, 2026
Strategic Compliance Training for Employees GuideOur strategic guide helps Canadian businesses develop effective compliance training for employees. Scope, build, deliver, & measure impactful programs for 2026.
Read Full Post
June 28, 2026
Vulnerability Assessment Services: Secure Your CanadianExplore vulnerability assessment services. Learn types, processes, & how to choose a provider to secure your Canadian business & meet compliance.
Read Full Post
June 27, 2026
Cloud Data Protection: A Complete Guide for Canadian SMBsProtect your business with our complete guide to cloud data protection for Canadian SMBs. Learn about threats, compliance like PIPEDA, and technical solutions.
Read Full Post